
Cyclical Discomfort

I hope this to be a compelling, useful story as far as I can tell about women’s health. I’ve previously ventured into this topic area, but perhaps without appropriate personalization. It’s hard to personalize pain you haven’t suffered, but probably no man is far removed from the suffering of the women in his life, I’m no exception. I’m writing to female kith and kin whose ripples of pain have had and have me digging for better understanding. I’m also writing to other men who are also hurt deeply by the state of the socio-biologic system we find ourselves in. I hope as much as I am able, that we may wake up to both the perversity of our status quo and wake up to the insight and potential for agency to turn it all around. Nature has laid down the rules for us to seek from which we can cast off of our ignorance.
Women’s cycles and fertility are temperature expressive and dependent. The metabolic and temperature frameworks I’ve written about in, The Heat of Attachment, Winter, Thyroid and Cardiovascular Health set the groundwork for understanding. However; the physiology of menstrual cycles is a place of important dynamics to learn from and is likewise rich for applications of the foundational principles.
A very large and rapidly growing percentage of the female population suffers from pain, inflammation and potential fertility issues associated with menstrual endocrine dysregulation. While this is surely to be in evidence for some women in some cases of evolutionary history, it is very likely at a maximum for absolute and relative amounts in the current environment. Menstrual suffering is very likely surging similar to what we see in the CDC tracking of obesity. That is it was very rare and is now the new normal. However, it is almost certainly a much less discernible issue. No one really knows if their experience is “normal” and the health system seems to support only interventions that are palliative with the potential escalation to surgical removal. Which seems a barbaric example for the professions lack of knowledge. What our health professionals might aim for as physiologically ‘normal’ in today’s environment is evolutionarily abnormal. And another ready answer for most MDs is likely to be use of some type of contraceptive or NSAIDs. Finding a contraceptive might be a way to some relief but not without some relatively silenced side-effects (see The Pill Changes Everything for more details).
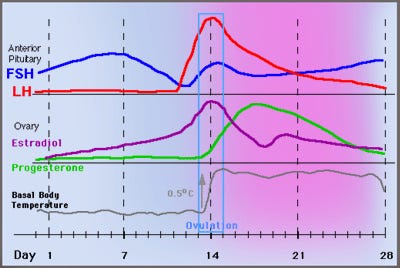
Estrogen acting through the body is associated with dissipating energy through vasodilation, while progesterone is associated with the core body temperature rising. While much of the reproductive literature seems mired in confusion and subterfuge the temperature basics are very clear. Estrogen concentration increases and drops the body temperature and while progesterone increases the body temperature also increases. They both act on temperature by modifying the amount of available active thyroid. Estrogen increases proteins that bind and block thyroid, while progesterone promotes more free thyroid. The temperature chart over the cycle is quite consistent with that story. The most energetically demanding period is when the core temperature and overall metabolism is increased and estrogen is both behaviorally and physically giving off heat.
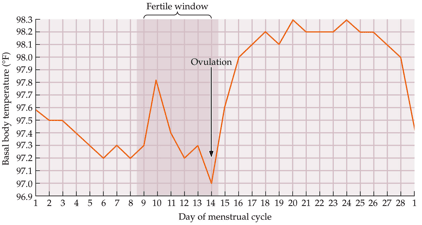
It’s no surprise that this occurs just at ovulation. In the chart below you can see that estrogen increasing drives the low temperature and the progesterone increase is consistent with the increase in temperature.
Where it gets a little murky is with the cause of premenstrual mood and bodily sensation. With a perspective related to thermoregulation and metabolism we can put together the picture being hidden. Many official sounding sources seem to implicate progesterone in increasing PMS symptoms which I think is probably (almost certainly) wrong and runs counter to many other practitioners using progesterone to alleviate the very same menstrual symptoms. Given what we know about heat and thyroid association with progesterone, I think those anti-progesterone ideas are generally inconsistent. Much of the confusion seems to come from studies not discriminating between actual progesterone and the various progestins invented to make money off the same actions a nonpatentable hormone progesterone does better, progestins like methoxyprogesterone.
To clear up the confusion here are pieces of the puzzle laid out:
From work on thermoregulation we know that a loss of body heat will drive a desire to seek out heat, calories and connection, a lack of body heat feels a lot like loneliness.
The symptoms of hypothyroid are remarkably similar to symptoms of premenstrual syndrome: stress, overwhelm, depression, tearfulness, mood swings, ease to anger
High cortisol production competes with progesterone for production, but unlike progesterone which causes steady blood sugar, cortisol causes swings in blood sugar and reduces insulin, and insulin sensitivity. Cortisol allows the body to use glucose, protein and fat rapidly for highly immediate stress response.
Sufficiently high progesterone is necessary for the next cycle’s estrogen receptor sensitivity to be reset, lack of which can further increase estrogen imbalance
Anecdotes from those who manage their own work schedules suggest that taking one to two days off work, reducing stress, coincident to when PMS or cramping would occur, seems to dramatically reduce if not eliminate pre and menstrual symptoms.
Many functional MDs and naturopaths use bio-identical progesterone or vitex during the luteal phase to ameliorate symptoms of PMS and menstruation.
Vitex increases luteinizing hormone, progesterone and dopamine while reducing estrogen, prolactin, and follicle stimulating hormone.
Real progesterone is a precursor to allopregnanolone.
Allopregnanolone is one of the most important hormones promoting positive mood and has relaxing and soporific effects.
Progesterone is known to reduce inflammation, reduce prostaglandins, inhibit endometrial growth and thin and stabilize the endometrium.
Cortisol production increases prostaglandin production while progesterone decreases it
Progesterone is used to treat endometriosis.
When less endometrium is grown, bleeding is less and removal is more complete
Increasing metabolism for a sustained increase in temperature and reducing cortisol requires an increase in energy from the diet after ovulation.
Cortisol and insulin are antagonists, meaning higher carbohydrates would reduce cortisol and so too prostaglandins along with premenstrual and menstrual symptoms
Omega-6 oils are extremely supportive of prostaglandin synthesis which helps reduce thyroid and prepares mammalian bodies for hibernation (see Winter, Thyroid and Cardiovascular Health)
Negative menstrual symptoms are highest when heat, thyroid, vitamin D, dopamine and progesterone are the lowest (Dec-Feb) in the northern hemisphere
What I think is going on follows. Firstly, premenstrual and menstrual issues seem to affect all women with variations of factors including age, bodily stress and inflammation, contraceptive use, and child status. Certainly genes also play a role, but the environment is so impactful and potentially unsupportive that we have a lot of options to exhaust before defaulting to a “bad genes” explanation. “Genes” is an easy go to for MDs who have no time to looking into research outside the pharmaceutically funded training courses. Also note that normal physiology in this decade of this century is not a good approximation of health status. Bodies are being attacked from multiple angles and it is highly likely that women are, on average, more sensitive to environmental conditions in order to unconsciously prevent investment in children when the environment is not conducive.
Most work environments, including white collar ones, require a kind of constant vigilance that is probably not good for anyone, but will most influence those people that are more physiologically sensitive. The modern economy has also done much to disrupt the kinds of social bonds that humans depend on, and lacking those we should expect some anxiety as a new baseline. Simultaneously, various chemicals and lifestyle factors are driving estrogen dominance while the entire food supply system is focused on delivering ever more of the least quality, most inflammatory calories. All of these and more are working together against all of our well being.
Applications
Taking or applying exogenous progesterone is something that I recommend to balance out the environmental deficits. Increasing one's active thyroid along with the increased calories to match is another good option. Many people are hypothyroid which leads to limited hunger and even the metabolic processes for proper digestion. I even do both progesterone and thyroid, even though menstrual management for me is irrelevant. Oxytocin is suggested in some of the literature for PMS and it’s more severe form PMDD. Taking oxytocin is perfectly consistent with metabolic-thermoregulatory perspective. Oxytocin increases peripheral metabolism and feels like, from both the literature and personal experience, more confidence or less social insecurity. Cannabinoids THC-a and CBD are also suggested to be beneficial as anti-inflammatories and their potential for reducing stress. All of that said, the first place we should probably consider focusing our efforts is electrolytes.
I have been amazed to find potassium as a ready solution for dysmenorrhea. 400 - 600mg of potassium gluconate daily and apparently the dysmenorrhea should disappear during the second cycle after starting. There is a lot more to learn about potassium, but that is a very cheap and ready option for those willing to venture a try. Evolutionary peoples almost certainly ate much more potassium than we do. Magnesium has some evidence behind it and should be managed for all types of health ailments including menstruation. Proper amounts of both magnesium and potassium will reduce blood pressure. Premenstrual discomfort seems significantly related to the body's water balance and blood pressure as it comes with a rise in blood pressure of 20 -30 mm and associated water retention. Both potassium and progesterone oppose cortisol. Cortisol like aldosterone is sodium retaining and potassium excreting, and opposing it increases the balance towards sparing potassium and excreting sodium. Water will go along with the sodium as will much of the swelling and increased blood pressure. The body will also return to a more insulin sensitive and reduced stress state. Below is a diagram of potassium’s immediate effects including reducing sympathetic nervous system and increasing the metabolism through insulin excretion and vasodilation:

Below is a report from someone who self treated her PMDD:
“Eating a potassium-rich diet, which I had always done, did not help my symptoms.
I knew taking potassium supplements was medically safe for me, so I began taking them every day beginning very early in my cycle. To my surprise, my stamina and energy level dramatically improved. This occurred within the first week of beginning the potassium when it was still my non-symptom follicular phase. In retrospect, I had become so accustomed to my stamina being low all the time that it seemed normal compared to the extreme fatigue I experienced during my PMDD time. Over the next three months, my symptoms gradually decreased until I was completely free of PMDD.”
Seems kind of miraculous but when considering the concentration of potassium in living cells and the food supply’s perpetual move towards delivering less and less fresh cells be they from meat, dairy, fruits or vegetables. All perishable foods have potassium because potassium is retained in the interior of cells as part of the living state’s energy management system. Making processed food essentially breaks or denatures cells and injury leads to a rapid loss of ATP and potassium. Top foods high in potassium include: greens, potatoes, milk, white button mushrooms, bananas and salmon. While doing this research I am taking at least 600 mgs daily of potassium gluconate - while also being cautious about using NSAIDs which can retain potassium and cause hyperkalemia. So far I only notice that my blood pressure is lower as is my blood sugar and I suspect it takes time to adjust down the insulin response to food with a higher potassium diet.
Behavioral:
I’ve heard very reliable anecdotes from friends who have completely mitigated the physical and emotional distress around menstruation by simply not working and taking the premenstrual days a bit easier. This makes lots of mechanistic sense as reducing cortisol and minimizing the calorie deficit that can easily kick in after ovulation when the body actually heats up to keep the potential bun warmer. Some countries like Japan, and a few companies like Nike actually seem to have some sensible policies around this. I was quite surprised in fact. I imagine however, that all of my readers will not have known a work environment beyond sole proprietorships that make this easy. Other ideas I’ve seen include increasing touch and physical intimacy for the oxytocin as mentioned briefly above. To be mildly cynical and hopefully slightly humorous, in experience, confidential notes from other men, and cultural lore it seems the lack of awareness or concern for the whole causal scheme depicted above as well as projection of the felt discomfort onto unwitting proximal subjects drives the likelihood of this type of physical intervention towards zero. From a partner’s point of view, it’s probably best to get the discomfort down through the appropriate metabolic inputs as an initial step.
Some Realted Products:
KrampAid - up to 4 grams of potassium!
OvuFirst™ Wearable Fertility Monitor - Starter Pack
Selected References:
The Purpose of Potassium – Dr.Berg
https://doi.org/10.1016/B978-0-323-43044-9.00166-7
https://europepmc.org/article/med/32789612
https://www.myfooddata.com/articles/food-sources-of-potassium.php
“After the intervention, the mean score of PMS significantly decreased in all the three groups (p < 0.05). The decrease was the greatest in the Mg plus vitamin B6 group, and was the least in the placebo group.”
Potassium: A New Treatment for Premenstrual Syndrome - Beckie E. Takacs, MS
evolutionary biology of endometriosis | Evolution, Medicine, and Public Health | Oxford Academic
“Premenstrual tension was aptly described by Dr. HE Billing in 1953 as irritability, depression and lethargy. “ Katerina Dalton MD 1969, The Menstrual Cycle
“Characteristically, patients with premenstrual syndrome have more than one symptom. Apart from tension..commonest symptoms include are headache, asthma, hay fever, joint and muscle pain and backache” Katerina Dalton MD 1969, The Menstrual Cycle