
Winter, Thyroid & Cardiovascular Health
Winter, Thyroid & Cardiovascular Health
Metabolic Applications

“Nothing in Biology Makes Sense Except in the Light of Evolution" Theodosius Dobzhansky
“Winter is coming” Ned Stark
We can only see the world through models. We are always projecting and looking for the error, and only where we look for error can we improve our models. If our models are too vague or low resolution the errors will not show up. If we define ourselves with loyalties to static models required for in group status and membership we will willfully blind ourselves to errors. I find the model I’m about to describe incomplete, but useful enough that I feel compelled to share it. I’m hoping to set the context for how I look at cardiovascular disease.
Modeling from Metabolism
The metabolic model I am building rests on a foundation of physics and computation. Metabolism in my view precedes biology and biological evolution. As beings in the world, we are subject ultimately to the laws of physics, and in my view the most relevant to our understanding of the processes of life is the second law of thermodynamics: All closed systems tend toward entropy (disorder). Within the universe’s race towards disorder, structures that allow life emerge far from energy equilibrium and facilitate faster entropy over energy gradients. In this prebiological way, metabolism is required for order and structure. Some of these emergent structures fell into a pattern of self replication and emergent life began evolving when and only when it continued to find and utilize energy for its perpetuitive purposes.
Our biosphere on earth is sitting in the light-energy field of our sun, and most of life flows from its radiance. For all of life, energy acquisition and utilization is critical for maintaining structure and for engaging pursuits in the world. The changes in sunlight through the seasons of our planet have a profound effect on how many species, including ours, are able to access the energy required to sustain life.
Winter adaptations
When I think about most types of disease, I first aim to remove as much of the internal and external signaling of winter we are layering into ourselves. Winter requires a number of adaptations that reduce our short term risks of death from freezing, disease and starvation. We want to move from having highly viscous blood to having lower resistance blood, lower inflammation, and increased peripheral metabolisms. This move towards repair, and reduced inflammation will generally require a higher energy throughput. Of course, having blood too thin increases some risks such as the risk of bleeding to death during trauma and we don’t want to get hyperthyroid or hyperthermia for their associated negative outcomes. However, from the average modern person's physiological status we can assume a reasonable amount. Most of us are running cold, with too little metabolism and too much stress. To our budgeting brains experiencing stress there is no distinction as to whether our caloric throughput is low or our external demands are too high. They are mutually defined, but typically we only consider the external stressors rather than our capacity to turn up our internal chemical fires.
When we prepare for winter or age our triiodothyronine (T3) levels decline. During that process we should expect to have excess cholesterol. Without T3 we will not convert our cholesterol into the sex hormones that signal repair and motivate reproduction and related productive behaviors. The reduction of UV, the metabolic slow down, and the decreases in social distances during fall and winter drive also pathogen spread1. The physiological preparations for winter increase inflammation through multiple pathways in order to pre-empt the pathogens and make blood less susceptible to freezing. We, like all organisms, expect it will be winter by attending to various environmental signals: the photoperiod, the temperature, and the composition of our diet.
I think the range of signals is still in flux, but we know of some signals. For example, polyunsaturated fats have proven to be strong signals telling mammals to put on the winter weight and increase inflammation2. We would only encounter polyunsaturated fat signals when cold and photoperiod were starting to affect the plants and animals we consider food sources. Psychologically, we will experience inflammation as less willingness to expend energy and an increased desire to eat. This would be useful if we were going to face cold and starvation. If the inflammation is bad enough it will feel like winter blues or seasonal affective disorder (SAD)3. Logically the increased inflammation will exacerbate all other conditions with an inflammatory component.
In our modern lives we may never really go through any other seasons. From our physiology’s point of view, we are stuck in late summer, and early fall. Food, sun exposure, and low activity all tell us winter is coming. In our modern lives winter is always coming, and never arriving. Our photo periods are erratic, we never experience weight shedding from seasonal caloric deficiency and fasting, nor do we receive the diets which would signal spring or summer arrival. We miss important seasonal signals like increased vitamin D, vitamin K2 and the daily increasing nitric oxide from the sun on skin. Importantly, when we are preparing for winter we are increasing inflammation and cardiovascular damage and not engaging the required repair. Repair requires vasodilation and the nutrient calories and substrate proteins to form and grow.
Inflammatory signaling is a significant driver of the aging phenotype. As we age we reduce the production of hormones and triiodothyronine is one of critical regulators whose production drops off4. As I see it, until we have a sufficient protocol to turn back the aged phenotype to a definitively younger state, it makes sense to return to the hormones and other signals of youth and late spring. Likewise, we should do that while reducing or blocking signals of aging and inflammation.
Statins
The ‘pro-statin’ logic is one of metabolic reduction. Statins are supposed to work by blocking an enzyme such that it can no longer produce as much cholesterol. The side effects of the drugs are contentious with more and more momentum heading towards increases in risk of type 2 diabetes along with memory and cognitive impairments. The reduction in cholesterol from statins, from my point of view, is an undesirable side effect. And so far in my reading of the research most of the claimed benefits are communicative artifacts5. It is possible some people benefit from the anti-inflammatory properties of statins. However, if the pharmaceutically backed researchers changed the target for cardiovascular disease (CVD) to a target of chronic cardiovascular inflammation they would put statins out of the market. There are many anti-inflammatories with better economics and lower risks.
One of the least difficult and expensive interventions to keep up the internal thermostat is to supplement thyroid back to youthful levels. Active thyroid - triiodothyronine (T3), is the central regulator of cellular metabolism, and seems to be cardio restorative6. Modern medicine, conveniently, has forgotten about thyroid and its relationship to cholesterol and cardiovascular disease.
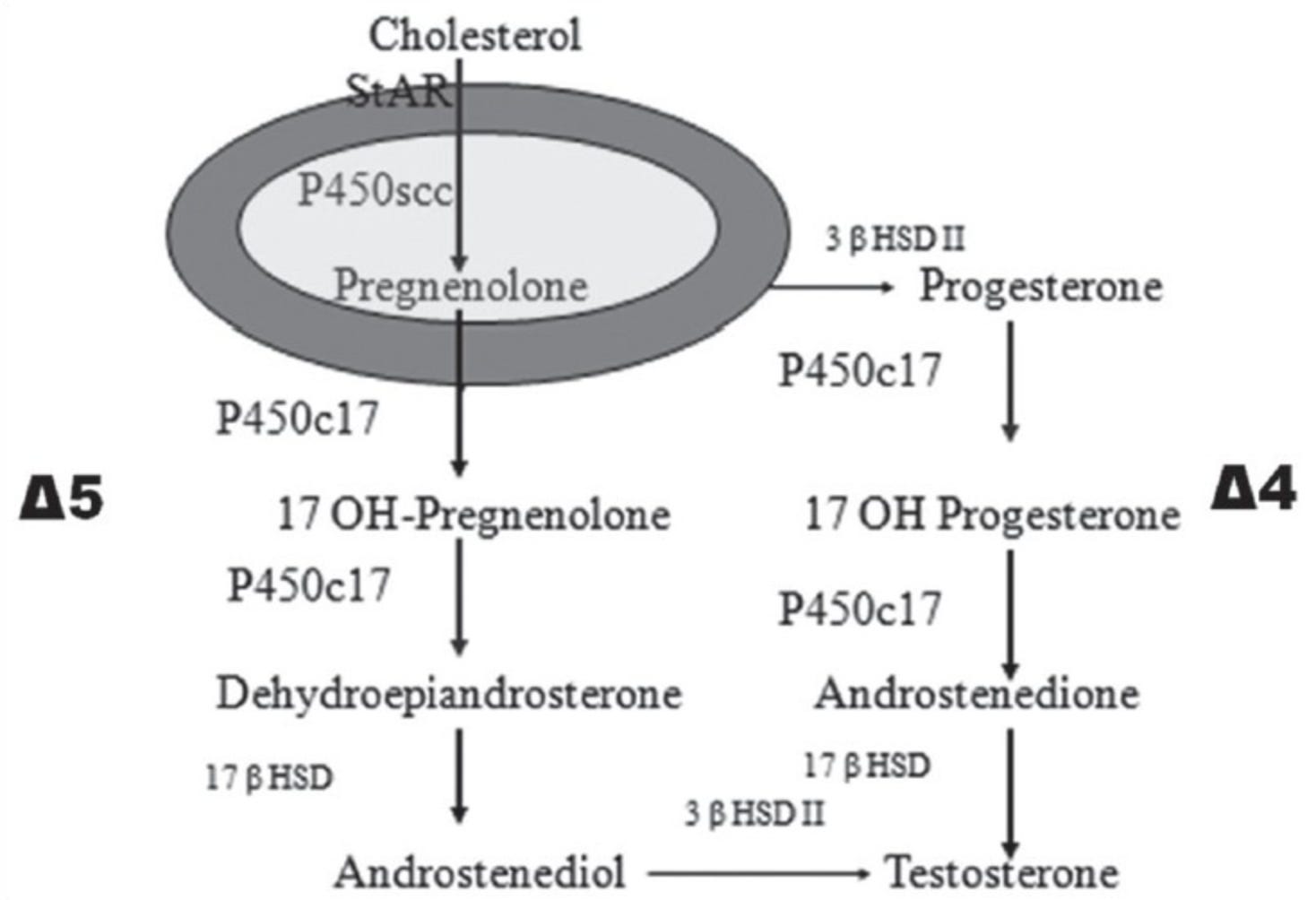
Steroid Cascade
When we are young adults we produce lots of sex hormones from...cholesterol7. A main throttle for that production is T3. Most of the hormones formed from cholesterol are mediators of inflammation8. Here is the steroid biosynthetic pathway:
In this study: Thyroid and male reproduction9 they clearly lay out the influence of thyroid on activating the steroid production process.
Firstly, T3 increases the cells that produce steroids:
“T3 facilitates the differentiation of mesenchymal stem cells into Leydig cells.[22]”
And T3 facilitates the production of pregnenolone:
“T3 treatment for 30h shows a significant increase in P450scc enzyme responsible for catalyzing the conversion of cholesterol to pregnenolone,”
then T3 drives the sex steroid production from precursors:
“T3 stimulates testosterone production by goat Leydig cells in a dose dependent manner.”
Reduction of T3 clearly also impairs production and sexual function:
“Removal of thyroid glands in albino rats completely inhibited the contractile activity of vas deferens”
“In hypothyroid males we found a significant decrease in gonadal steroids – progesterone and total testosterone. Bioavailable testosterone (BioT) or physiologically available testosterone, calculated by Morris's formula,[54] was also reduced in hypothyroid men”
For the heart, thyroid seems to directly turn back the clock phenotypically, along with reducing blood pressure and inflammation.
“Thyroid hormones have many cardioprotective actions expressed mainly through the action of T3 on thyroid receptors α1 and β1. They are procontractile anti-apoptotic, anti-inflammatory, and anti-fibrotic, promote angiogenesis and regeneration, and have beneficial effects on microRNA profiles” “Remodeling can be defined as an increase of ≥20 % of the end-diastolic or end-systolic volume, together with a return to the fetal phenotype.”
Comparing views
If we were forced to constrain ourselves to these two options: thyroid or a statin, we would have either: a statin that is probably anti-inflammatory to some degree, but lowers sex steroid production with reducing effects on energy balance, cognition and repair of tissues or thyroid which is anti-inflammatory and causes the production of a variety of anti-inflammatory gasses and molecules. It does this while increasing the systemic usage of fats and sugars resulting in lower body fat, higher temperatures, higher feelings of energy, and significantly increased cognitive blood flow.
Substructures of morality
Taking a step back and being a bit playful, I find the standard medical approach to managing CVD perfectly aligned with a kind restriction harkening back to puritanism, or even further back to when social class and reproductive biology were inextricably linked. It’s as if the reduction in physical and cognitive vitality is actually the desired end-state. Yet, I imagine the agents in the system are taking their own medicine literally, so it’s a bizarre coincidence. Perhaps the coincidence relates as well to some fundamental principle of life which beyond acquiring energy requires a kind of openness. Cholesterol as a fundamental component to expressing vitality seems consistent with the metabolic framework around allowing emotions to emerge and exit. Learning how to appropriately express emotions happens to be fundamental to being well10. The body budget model makes the logic clear. We use and lose so much extra energy suppressing or distracting ourselves from how we feel that reducing suppression gives us a future energy dividend we can use to better adapt to the world. Of course, competitors for status, resources and reproduction would prefer it if you didn’t.
How to pursue
If you like this point of view and go to a regular doctor you might need to bring a notebook of research and you will need to suggest that the reference range for thyroid stimulating hormone (TSH) is too wide. You’d like to be biased towards hyperthyroid. Getting evaluated against the norms of the population of Americans getting blood work will significantly biased your doctor towards maintaining hypothyroidism. While the upper boundary of normal TSH is supposed to be around 4 mIU/L, practitioners sometimes want to wait until a TSH as high as 10 mlU/L. Personally, I want my TSH down to or below 1 mlU/L. In the framework of aging this should make sense. We want to keep as much of the peripheral tissues supplied with oxygen and nutrients as long as possible. Hopefully this essay and the links below are sufficient to drive a productive discussion with your doctor.
Assuming you have a nonstandard doctor, they will hopefully test your thyroid levels beyond TSH. TSH can be misleading and blood triiodothyronine is quite variable and distinct from the tissue conversion of thyroxine (T4). Ideally, they will pay attention to your symptoms: temperature (core and peripheral), energy and mood, bowel ease etc.
One of the many things thyroid will do is relax and regularize bowel movements, not unrelated to the push of blood and energy to the digestive system. The increased frequency of bowel movements while on thyroid will also help reduce the ability of unwanted microbes from taking over parts of the intestine.
Suggestions:
Beyond my position on statins and thyroid I have a number of less controversial suggestions to investigate for CVD:
eNO precursors (do 1 or some, I’m not suggesting all at the same time):
Recall that aerobic metabolism and CO2 production is an eNO precursor
So too is exercise
L- Citrulline
Dried Beet Powder
Resveratrol - this one seems the most likely to reverse the sclerotic build up.
Cialis/Viagra (PDE5 inhibitors)
Oxytocin - see Oxytocin
Sun Exposure*
*NO precursors pair well with getting daily red, infrared or sunlight which will release NO into the vascular tissue causing relatively immediate relaxation.
Other useful options/ideas:
Vitamin D - among many things D is an inhibitor of Thrombin, but it needs to be taken with significant Vitamin K2
Vitamin k2 mk4 & mk7 - Mk7 is shown to be rather more efficient than mk4 at reversing calcification in plaque. We assume this is consistent with endothelial healing, but mk4 is associated with reduction in all cause mortality so I would suggest both.
Vitamin C
Magnesium Threonate or citrate
Aspirin (crushed and dissolved)
Pregnenolone (for men)
Pregnenolone and progesterone (for women)
DHEA
Spermidine
Haemophilia - perhaps only donate blood.
Alpha Lipoic Acid (ALA)
References:
Intensive Lifestyle Changes for Reversal of Coronary Heart Disease
“These findings support the feasibility of intensive lifestyle changes in delaying, stopping, or reversing the progression of coronary artery disease in ambulatory patients over prolonged periods.”
I don’t like the above method of reducing CVD, but it shows the feasibility without statins.
Inflammation:
Inflammation, not Cholesterol, Is a Cause of Chronic Disease
“inflammation induced by several factors, such as platelet-activating factor (PAF), that leads to the onset of cardiovascular diseases (CVD) rather than serum cholesterol. The key to reducing the incidence of CVD is to control the activities of PAF and other inflammatory mediators via diet, exercise, and healthy lifestyle choices.”
“after age 50 years there is no increased overall mortality with either high or low serum cholesterol levels.”
Lipid lowering drugs and inflammatory changes: an impact on cardiovascular outcomes
“patients achieving on-treatment hsCRP concentrations ≤2 mg/L had a higher benefit in terms of reduction in major CV events”
“Statin treatment results in a surprisingly small average gain in overall survival within the trials’ running time.”
“ The dose dependent cognitive impairment relationship reported in the atorvastatin safety study suggests that high doses cause cognitive side effects.”
Thyroid:
The Effect of Endocrine Disorders on Lipids and Lipoproteins
Mechanism of Action and Physiologic Effects of Thyroid Hormones
Thyroid hormones and the metabolic syndrome
Low-normal thyroid function and the pathogenesis of common cardio-metabolic disorders
Thyroid hormones and the metabolic syndrome
Thyroid hormone and cardiovascular disease
Thyroid hormones and cardiac remodeling
The History and Future of Treatment of Hypothyroidism
Treating Thyroid patients like children
Nitric Oxide precursors11:
l-Citrulline Supplementation: Impact on Cardiometabolic Health
“Collectively, these studies in diverse animal models have demonstrated the critical role of NO in endothelial protection against atherogenic dietary conditions”
Resveratrol_in_Cholesterol_Metabolism_and_Atherosclerosis
The Potential Benefits of Red Beetroot Supplementation in Health and Disease
Phosphodiesterase-5 Inhibitors and Survival in Men With Coronary Artery Disease
“Erectile dysfunction (ED) predicts future cardiovascular events in men” - I put this here to point out the equality of reproductive health and overall health.
The Effects of Resveratrol in Patients with Cardiovascular Disease and Heart Failure
Resveratrol and Its Effects on the Vascular System
Role of Nitric Oxide in the Cardiovascular and Renal Systems
Vitamin C & Vitamin D
Hypoascorbemia induces atherosclerosis and vascular deposition of lipoprotein(a)
Vitamin C inhibits the calcification process in human vascular smooth muscle cells
Magnesium:
Low magnesium and atherosclerosis: an evidence-based link
Lipoic Acid:
Lipoic acid effects on established atherosclerosis
“demonstrated that LA reduced atherosclerotic plaques in the abdominal aorta”
Spermidine:
Higher spermidine intake is linked to lower mortality: a prospective population-based study
K2
Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: the Rotterdam Study Note: Intake of menaquinone was also inversely related to all-cause mortality
The Bone—Vasculature Axis: Calcium Supplementation and the Role of Vitamin K
“In particular, VitK2 deficiency seems to be responsible for the so-called “calcium paradox” phenomenon, characterized by low calcium deposition in the bone and its accumulation in the vessel wall”
DHEA (and Testosterone)
Plasma Dehydroepiandrosterone Sulfate and Cardiovascular Disease Risk in Older Men and Women
Dehydroepiandrosterone anti-atherogenesis effect is not via its conversion to estrogen
General
Does diet play a role in cardiovascular disease? - Dr Malcolm Kendrick
Posted in Cardiovascular Disease
What Causes a Heart Attack? | Dr Malcolm Kendrick | Ep 17
Dopico, X., Evangelou, M., Ferreira, R. et al. Widespread seasonal gene expression reveals annual differences in human immunity and physiology. Nat Commun6, 7000 (2015). https://doi.org/10.1038/ncomms8000
““PUFAs, but not of n-3 PUFAs, can strongly enhance the propensity for hibernation, and allows heterotherms to reach lower body temperatures, with associated increased energy savings.” Ruf T, Arnold W. Effects of polyunsaturated fatty acids on hibernation and torpor: a review and hypothesis. Am J Physiol Regul Integr Comp Physiol. 2008 Mar;294(3):R1044-52. doi: 10.1152/ajpregu.00688.2007. Epub 2008 Jan 2. PMID: 18171691.
This is also related to blue light timing and circadian dysregulation resulting in inflammation. Bedrosian TA, Nelson RJ. Timing of light exposure affects mood and brain circuits. Transl Psychiatry. 2017;7(1):e1017. Published 2017 Jan 31. doi:10.1038/tp.2016.262
Mohanty SK, Suchiang K. Triiodothyronine (T3) enhances lifespan and protects against oxidative stress via activation of Klotho in Caenorhabditis elegans. Biogerontology. 2021 Aug;22(4):397-413. doi: 10.1007/s10522-021-09923-0. Epub 2021 Apr 13. PMID: 33851304.
Trail authors for highly profitable chemicals seem to use a variety of methods to bamboozle journalists and the public. Namely highlighting relative risk vs absolute risk. Here is an example described in a paper critiquing the JUPITER trial which suggested that almost everybody should go on statins: “These rates translate into an absolute risk reduction of about a half percentage point per year (0.59%), or 1.2% over the approximately 2-year total duration of the trial. This figure is obviously much less impressive to the casual reader than the relative risk reduction of 44%.” A 44% relative risk reduction is almost zero absolute risk reduction (from primary endpoints only).
Cokkinos DV, Chryssanthopoulos S. Thyroid hormones and cardiac remodeling. Heart Fail Rev. 2016 Jul;21(4):365-72. doi: 10.1007/s10741-016-9554-7. PMID: 27138258.
See: Count Down (Swann 2021) for why that may no longer be true
Lichte P, Pfeifer R, Werner BE, et al. Dehydroepiandrosterone modulates the inflammatory response in a bilateral femoral shaft fracture model. Eur J Med Res. 2014;19(1):27. Published 2014 May 19. doi:10.1186/2047-783X-19-27
Kumar A, Shekhar S, Dhole B. Thyroid and male reproduction. Indian J Endocrinol Metab. 2014;18(1):23-31. doi:10.4103/2230-8210.126523
When the Body Says No (Mate 2003), All Chapters
We really only want to increase endothelial and perhaps neuronal Nitric Oxide. Nitric oxide has a few pathways associated with increasing inflammation that help with immunity. Nitric oxide synthase